Improvement of cardiac sympathetic nerve function in sarcoidosis
Nanda M. Smulders1, Aalt Bast2,4 , Marinus J.P.G. van Kroonenburgh (m.van.kroonenburgh@mumc.nl)1,4, Marjolein Drent 3,4
1Dept of Nuclear Medicine, 2Dept of Pharmacology and Toxicology, 3Dept of Respiratory Medicine, 4ild care centre, Maastricht University Medical Centre (MUMC), The Netherlands
Background
Sarcoidosis is a multi-organ inflammatory disorder of unknown origin and the development of granulomas is the fundamental abnormality. The clinical manifestations of sarcoidosis are highly variable and many organs can be involved [1]. Besides pulmonary symptoms many patients suffer from fatigue, pain and autonomic dysfunction. Recently, we found that small fiber neuropathy (SFN) appeared to be rather common in sarcoidosis patients [2]. Moreover, about 50% of patients with small fiber neuropathy showed impaired cardiac sympathetic nerve activity what can be assessed by iodine-123 metaiodobenzylguanidine (I-123 MIBG) [3].
Objective
To describe a sarcoidosis patient with impaired cardiac sympathetic nerve function which improves after carvedilol therapy.
Methods and Findings
A 48 years-old man known with pulmonary sarcoidosis (disease duration 5 years) and small fiber neuropathy presented with cardiac arrhythmia and dizziness since two weeks before admission. Inflammatory parameters of sarcoidosis were slightly increased compared to three months earlier. Because of the cardiac symptoms the cardiac sympathetic nerve function was assessed by myocardial SPECT imaging with the use of radiolabeled I-123 MIBG. The images demonstrated absent uptake of I-123 MIBG in the apical inferior wall of the myocardium (Figure 1a). Bulls’ eye quantification showed a defect size of 16.3% (Figure 1b). A myocardial perfusion SPECT scintigraphy with Thallium-201 showed normal perfusion in the apical inferior wall. Echocardiography and MRI of the heart were also judged normal. He was treated with carvedilol for five months and his clinical condition stabilized and no activity of sarcoidosis could be found. He did not recall heart rhythm disturbances anymore. The I-123 MIBG SPECT study was repeated and showed improvement of the uptake in the apical inferior wall (Figure 1c), with a defect size of only 3.9% (Figure 1d).
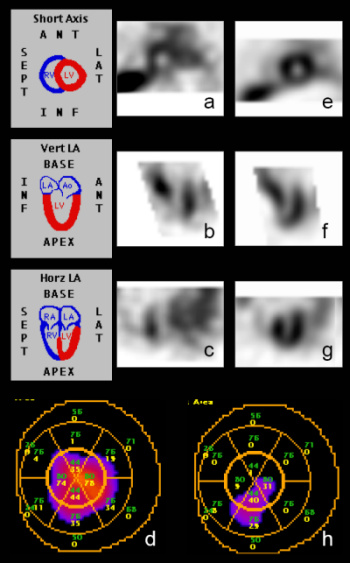
Figure 1 I-123 MIBG SPECT acquired 4 hours after tracer injection with absent uptake in the apical inferior wall (a, b, c), with a quantification of 16.3% (d). Marked improvement of the uptake in the apical inferior wall after carvedilol treatment (e, f, g), with a quantification of only 3.9% (h).
Discussion
In patients with dilated cardiomyopathy it was demonstrated that the cardiac sympathetic nervous system function can improve in response to carvedilol therapy [3]. Besides a selective antagonist effect on alpha 1- adrenergic receptors, thereby decreasing the total peripheral resistance, and a cardiac nonselective beta – adrenergic receptor blocking action, thereby preventing reflex tachycardia, carvedilol has a potent antioxidant action [4,5]. Sarcoidosis has been suggested to trigger an oxidative stress response as indicated by an increased activation of NF-κB [6].
This case provides clinical support that oxidative stress may contribute to cardiac dysfunction in sarcoidosis through increased susceptibility to free radical injury and impairment of intracellular calcium transport. Moreover, it illustrates improvement of cardiac sympathetic function in a sarcoidosis patient after 5 months of treatment with carvedilol. Future studies should explore the clinical relevance of the relation of oxidative stress and cardiac dysfunction in sarcoidosis.
References
Iannuzzi Mc, Rybicki BA, Teirstein AS. Sarcoidosis. N Eng J Med 2007; 357:2153-2165.
Hoitsma E, Marziniak M, Faber CG, Reulen JPH, Sommer C, Baets de M, Drent M. Small fiber neuropathy in sarcoidosis. Lancet 2002; 359: 2085-2086.
Hoitsma E, Faber CG, Kroonenburgh van MJPG, Gorgels APM, Halders SGEA, Heidendal GAK, Kessels AGH, Reulen JPH, Drent M. Association of small fiber neuropathy with cardiac sympathetic dysfunction in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 2005; 22: 43-50.
Flesch M, Maack C, Cremers B, Baumer AT, Sudkamp M, Bohm M. Effect of b-blockers on free radical-induced cardiac contractile dysfunction. Circulation 1999; 100: 346-353.
Drent M, Gorgels AP, Bast A. Cardiac failure associated with G6PD deficiency. Circ Res 2003; 93(8):e75.
Drent M, van den Berg R, Haenen GRMM, van den Berg H, Wouters EFM, Bast A. NF-?B activation in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 2001 ; 18 : 50-56.
Source: Smulders NM, Bast A, van Kroonenburg MJPG, Drent M. Improvement of cardiac sympathetic nerve function in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis; 2008: 25: 140-42.
Feedback & comments
If you would like to share any comments on this case please send them to wasog@gosker.nl and after peer review your comment(s) will be posted below.